
Pneumonia in Immunocompromised Patients
People with weakened immune systems are vulnerable to additional organisms, including:
- Pneumocystis jirovecii pneumonia (PCP) in HIV patients with CD4 counts <200
- Nocardia
- Non-tuberculous mycobacteria
- Fungal infections
These cases often require specialized testing and treatment.
How Pneumonia Is Diagnosed
Diagnosis is based on a combination of clinical assessment and investigations.
Initial Evaluation
- Review of symptoms and medical history
- Physical examination (listening to lung sounds)
- Measurement of oxygen saturation using pulse oximetry
Imaging
- Chest X-ray is the most important diagnostic test
- Lobar consolidation suggests bacterial pneumonia (e.g., Strep pneumoniae)
- Patchy interstitial infiltrates suggest viral or atypical pneumonia
Laboratory Tests
- Complete blood count (elevated white blood cells suggest infection)
- Sputum culture and Gram stain (before starting antibiotics)
- Blood cultures in severe cases
- Procalcitonin (may help distinguish bacterial vs viral infection)
- Viral PCR testing when viral pneumonia is suspected
- Arterial blood gas (ABG) in severe or hypoxic patients
Advanced Testing (Selected Cases)
- Bronchoscopy for severe or non-responsive cases
- Urinary antigen tests for Legionella
- HIV testing when immunodeficiency is suspected
Pneumonia Severity Assessment
Severity scoring systems help determine whether a patient can be treated at home or needs hospitalization or ICU care.
qSOFA Criteria (Quick Assessment)
Used for rapid risk assessment:
- Respiratory rate ≥22/min
- Altered mental status
- Systolic BP ≤100 mmHg
A score ≥2 indicates higher risk and need for urgent care.
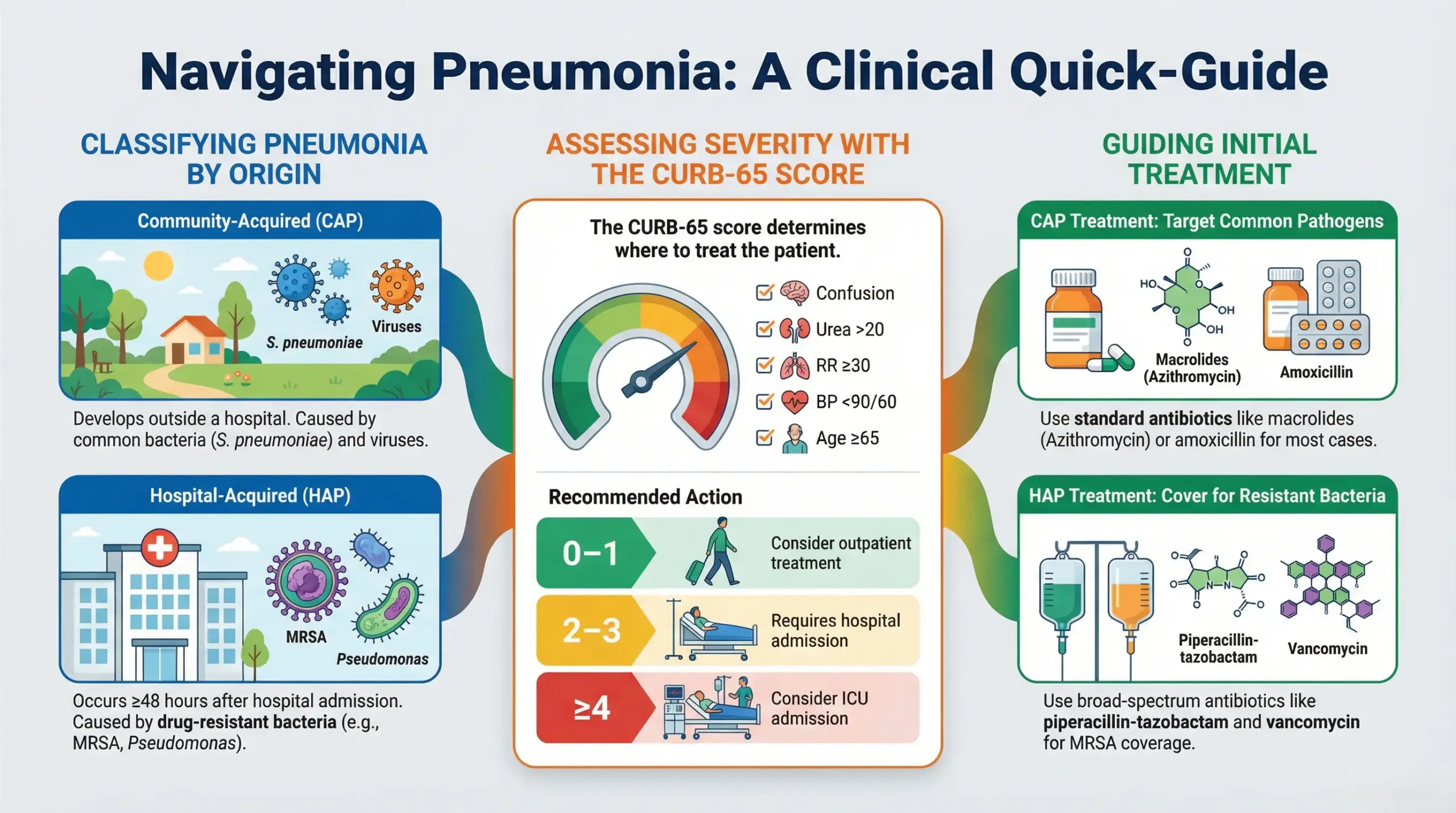
CURB-65 Score (Pneumonia-Specific)
- Confusion
- Urea >20 mg/dL
- Respiratory rate ≥30/min
- Blood pressure <90/60 mmHg
- Age ≥65 years
Interpretation:
- 0–1: Outpatient treatment
- 2–3: Hospital admission
- ≥4: ICU consideration
Treatment of Pneumonia
Treatment depends on the type, severity, and cause of pneumonia.
Community-Acquired Pneumonia
- Mild cases (outpatient):
- Azithromycin, doxycycline, or clarithromycin
- Azithromycin, doxycycline, or clarithromycin
- Moderate cases (hospitalized):
- Amoxicillin + macrolide
- OR respiratory fluoroquinolone
- Severe cases (ICU):
- Third-generation cephalosporin + respiratory fluoroquinolone
- OR beta-lactam + macrolide
Hospital-Acquired Pneumonia
- Broad-spectrum antibiotics targeting resistant organisms:
- Piperacillin-tazobactam
- Vancomycin (for MRSA)
- Carbapenems for resistant cases
- De-escalation once cultures identify the organism
Role of Steroids
Steroids are not routinely used, but may be considered in severe community-acquired pneumonia to reduce inflammation and complications.
Supportive Care and Recovery
Supportive measures play a crucial role in recovery:
- Oxygen therapy when needed
- IV fluids in hospitalized patients
- Incentive spirometry to improve lung expansion
- Adequate hydration to thin respiratory secretions
- Sitting upright and frequently deep breathing
Recovery may take weeks, and fatigue can persist for up to a month.
Preventing the Spread of Pneumonia
To reduce transmission and complications:
- Cover your mouth and nose when coughing or sneezing
- Wash your hands frequently
- Avoid close contact when ill
- Complete prescribed medications fully
Vaccination and Prevention
Pneumococcal vaccination is recommended for:
- Adults aged 65 and older
- Immunocompromised individuals
- People with chronic heart, lung, liver, or kidney disease
Vaccination significantly reduces the risk of severe pneumonia and complications.
Final Thoughts
Pneumonia is a complex but manageable disease when approached systematically. Early diagnosis, appropriate classification, and timely treatment significantly reduce complications and mortality.
If respiratory symptoms persist or worsen, timely medical evaluation is essential. You may also consult healthcare professionals online through platforms like the MedIQ app for guidance and early intervention.